Ingredients
- What are Trachea Diseases?
- What is Tracheal Stenosis (Tracheal Stenosis)?
- Strictures After Intubation and Intensive Care
- Tracheal Damage Due to Trauma and Burns
- Trachea Tumors and Types
- Benign Tracheal Tumors (Papilloma, Chondroma)
- Malignant Tracheal Tumors (Squamous Cell Carcinoma and Adenoid Cystic Carcinoma)
- Symptoms of Tracheal Diseases: When to Consult a Specialist?
- Diagnosis and Diagnostic Methods
- Bronchoscopy: Internal Examination of the Trachea
- Virtual Bronchoscopy and Dynamic CT Imaging
- Treatment Methods for Tracheal Stenosis
- Interventional Bronchoscopy: Laser, Balloon and Stent Applications
- Tracheal Resection and Anastomosis: A Definitive and Permanent Surgical Solution
- Surgical Approach and Oncological Treatment in Tracheal Tumors
- Postoperative Recovery Process and Things to Consider
- Frequently Asked Questions
- Is Tracheal Stenosis Confused with Asthma?
- How long should a tracheal stent stay?
- Is Tracheal Surgery a High-Risk Procedure?
The trachea, or trachea as it is medically called, is a vital conduit about 10-12 centimeters long that transports air from the outside world to the lungs.
Narrowing of the inner diameter of this canal or masses developing in its wall directly prevent the body’s most basic need for oxygen intake.
Since tracheal diseases are often confused with other respiratory diseases such as asthma or bronchitis, there may be delays in the diagnosis phase.
However, a mechanical obstruction on the trachea requires surgical or interventional intervention, unlike lung diseases that can be treated with medication.
Modern thoracic surgery treats strictures and tumors in this vulnerable area with advanced reconstruction techniques, restoring the patient’s breathing capacity.
What are Trachea Diseases?
Tracheal diseases are generally grouped into three main groups: structural stenosis, benign or malignant tumors and traumatic damage.
Conditions such as loss of flexibility of the airway (tracheomalacia) or the formation of unwanted connections between the esophagus and the esophagus (fistula) are also included in this scope.
What these diseases have in common is that they disrupt the tubular anatomy of the trachea, increasing airflow resistance.
Early detection is critical to halt the progression of tissue damage in the trachea and ensure recovery without the need for more complex surgical interventions.
What is Tracheal Stenosis (Tracheal Stenosis)?
Tracheal stenosis is the narrowing of the inner volume of the trachea due to scar tissue or external pressure.
Patients may usually not feel any obvious complaints until the airway diameter narrows by more than 50%; However, after this limit, severe breathlessness begins.
Stenosis can occur at any level of the windpipe and can sometimes extend just below the vocal cords (subglottic region).
Strictures After Intubation and Intensive Care
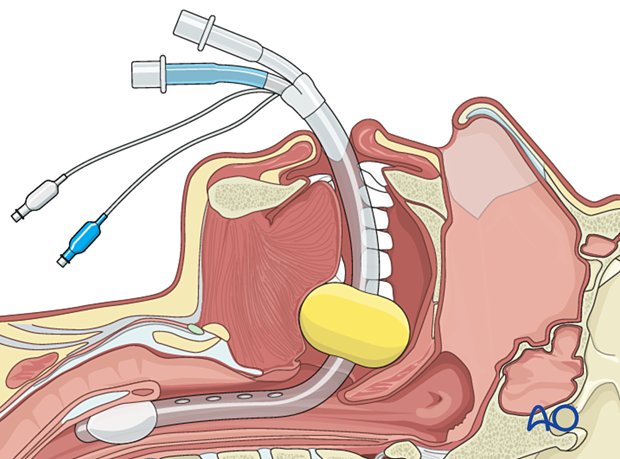
Today, the most common cause of tracheal stenosis is the long-term process of being connected to a ventilator in intensive care units.
The bubble (kaff) of the tube placed in the trachea while connected to the device can put pressure on the trachea wall and prevent blood circulation there.
The tissue whose circulation is impaired shrinks as it heals and narrows the canal by forming a hard scar tissue.
These patients usually begin to experience shortness of breath 2 to 6 weeks after discharge; It should not be forgotten that this condition is not “post-recovery fatigue”, but a mechanical stenosis.
Tracheal Damage Due to Trauma and Burns
Traffic accidents, hard blows to the neck area or penetrating injuries can cause permanent damage to the trachea.
In addition, very hot air or chemical vapors inhaled during a fire lead to deep burns to the tracheal mucosa and subsequent widespread strictures.
Strictures that develop after such acute damage are usually more complex and require urgent surgical planning.
Trachea Tumors and Types
Tracheal tumors are much rarer than lung cancer, but require rapid action due to their vital location.
Tumors can block the inside of the trachea like a stopper or narrow the canal by pressing from the outside.
Benign Tracheal Tumors (Papilloma, Chondroma)
Benign masses usually grow slowly and do not spread to other parts of the body; however, they are dangerous because they take up space in the trachea.
- Papilloma: They are masses that can usually be of viral origin and form wart-like structures.
- Condrome: They are hard formations originating from the cartilage rings of the trachea.
- Hemangioma: They are vascular masses and can cause coughing up blood.
Malignant Tracheal Tumors (Squamous Cell Carcinoma and Adenoid Cystic Carcinoma)
Most tracheal cancers are malignant and have a high chance of surgical treatment when caught at an early stage.
- Squamous Cell Carcinoma (SCC): It is often associated with smoking and tends to grow rapidly.
- Adenoid Cystic Carcinoma: It has a slower course but has the characteristic of progressing along the nerve sheaths; Cleaning of surgical margins is very critical in this type.
Symptoms of Tracheal Diseases: When to Consult a Specialist?
Symptoms usually depend on the level of stenosis and are very susceptible to confusion with other diseases.
If one or more of the following symptoms are present, a thoracic surgeon should be consulted:
- Stridor: A whistle-like, high-pitched sound heard when breathing.
- Shortness of Breath Increasing with Exertion: Feeling of congestion when climbing stairs or walking.
- Persistent Dry Cough: Persistent cough due to irritation in the trachea.
- Hoarseness: Masses or stenosis affecting the vocal cords.
- Hemoptysis: Coughing up blood from the mouth.
Prof. Dr. Levent Alpay: The most common mistake made in tracheal diseases is to confuse the stridor sound with “asthma wheezing” and give the patient unnecessary sprinkler treatment. If a patient does not feel relief despite asthma treatment or has a history of intensive care, the problem may be directly in the trachea, not in the lungs. Every day of delay in diagnosis can complicate the chances of surgery.
Diagnosis and Diagnostic Methods
Accurate diagnosis of tracheal diseases begins with determining the precise location, length, and relationship of the stenosis or tumor with surrounding tissues.
An erroneous diagnosis can lead to the wrong treatment method being chosen, leading to further damage to the airway.
Modern imaging and endoscopic systems provide the surgeon with a millimetric roadmap before surgery.
Bronchoscopy: Internal Examination of the Trachea
Bronchoscopy is the most critical method used for both diagnosis and treatment of tracheal diseases.
With the help of a thin, lighted camera, the trachea is entered and the internal structure of the canal is directly observed.
During this procedure, the degree of stenosis is measured, a biopsy is taken if there is a tumor, and the functional status of the airway is evaluated.
Virtual Bronchoscopy and Dynamic CT Imaging
Advances in Computed Tomography (CT) technology allow us to create a three-dimensional map of the trachea with a method called “Virtual Bronchoscopy”.
This method provides detailed images without any intervention to the patient, just as if they were walking around with a camera.
Dynamic CT is used to detect whether there is a collapse in the walls of the trachea (tracheomalacia) during breathing.
Treatment Methods for Tracheal Stenosis
The treatment plan is personalized based on the cause and length of the stenosis and the patient’s general health condition.
While closed methods may be sufficient in mild stenosis, surgery is inevitable in advanced stenosis.
Interventional Bronchoscopy: Laser, Balloon and Stent Applications
Interventional bronchoscopy is life-saving in patients who are not suitable for surgery or require emergency airway patency.
- Laser: It provides cleaning of excess tissues in the stenosis area by burning.
- Balloon Dilation: It is the controlled expansion of the narrowed area with special balloons.
- Stent Applications: They are silicone or metallic tubes that are inserted to keep the airway open.
However, it should not be forgotten that most of these methods are temporary solutions and there is a risk of recurrence of the stenosis.
Tracheal Resection and Anastomosis: A Definitive and Permanent Surgical Solution
The “gold standard” treatment method for tracheal stenosis is surgical removal of the narrowed part.
After the diseased area is removed, the two healthy ends are sutured together (anastomosis) to restore the integrity of the natural airway.
This procedure is the definitive solution that minimizes the risk of recurrence of the stenosis and ensures that the patient does not need interventional intervention again.
Surgical Approach and Oncological Treatment in Tracheal Tumors
The main goal of tracheal tumors is to completely remove the tumor tissue with clear surgical margins.
Depending on the type and stage of the tumor, additional treatments such as radiotherapy or chemotherapy may be planned after surgery.
Very successful results are obtained with tracheal resection in early-stage tumors and the patient’s life expectancy is significantly extended.
Postoperative Recovery Process and Things to Consider
The first few days after tracheal surgery are the most critical period for suture line preservation.
Patients are asked to restrict neck movements and avoid movements that will create tension in the stitches.
The recovery process is usually quick and patients can be discharged within a few days with easy breathing.
Comparison of Treatment Modalities and Recovery
| Feature | Interventional Bronchoscopy (Laser/Balloon) | Tracheal Resection (Surgery) |
| Purpose of Operation | Temporary relief / Emergency opening | Permanent and definitive treatment |
| Hospital Stay | Usually discharged on the same day | 5 – 7 Days |
| Recurrence | High | Very Low |
| Return to Normal Life | 1 – 2 Days | 2 – 4 Weeks |
Prof. Dr. Levent Alpay: Tracheal surgery is an art that requires millimetric precision. Every stitch placed during the surgery aims for the patient to breathe comfortably for life. Our priority is not only to open the stenosis, but also to protect the most natural anatomical structure without disturbing the blood supply to the tissue. For this reason, performing these surgeries in centers with experienced surgical teams and advanced intensive care support directly affects success.
Case Experience (Anonymous):
A 45-year-old patient, who was treated for asthma due to hoarseness and severe shortness of breath, was found to have a mass that blocked the upper part of the trachea by 85%. The tumor was completely cleared with a successful resection surgery. The patient regained a sigh of relief immediately after the surgery and returned to health without any damage to his vocal cords.
To determine the exact cause of your shortness of breath complaints and plan the most suitable treatment method for you, you can seek expert opinion and make an appointment with our clinic.
Frequently Asked Questions
Is Tracheal Stenosis Confused with Asthma?
Yes, the whistling sound called stridor in particular is very often confused with asthma wheezing; This can lead to incorrect medication use and delayed diagnosis.
How long should a tracheal stent stay?
Stents are generally used in patients who are not suitable for surgery or for temporary bridging; The duration is determined by the physician according to the cause of the stenosis.
Is Tracheal Surgery a High-Risk Procedure?
As with any major surgery, there are risks; However, with modern techniques and experienced hands, these risks are very low and surgery is the safest way for life-threatening strictures.
Scientific Bibliography
- The Lancet: Tracheal Stenosis: Diagnosis and Treatment Strategies
- The Annals of Thoracic Surgery: Long-term Results of Tracheal Resection
- PubMed (NCBI): Management of primary tracheal tumors
- Journal of Thoracic Disease: Interventional Bronchoscopy in Airway Obstruction
