Ingredients
- What is Shoemaker’s Chest (Pectus Excavatum)?
- Causes of Disease and Genetic Factors
- Shoemaker’s Chest Symptoms and Physical Effects
- Diagnostic Methods of Pectus Excavatum
- Physical Examination and Grading (Haller Index)
- Radiological Imaging: CT, MRI, and Echo Tests
- Evaluation of Heart and Lung Function
- Shoemaker’s Chest Non-Surgical Treatment Methods
- Vacuum Bell (Vacuum Therapy) Application
- Chest Wall Exercises and Physiotherapy Support
- Nuss Surgery (Closed Surgical Method)
- Ravitch Surgery (Open Surgical Method)
- The Most Suitable Age Range for Surgical Intervention
- Surgery Process and Recovery Period
- Preoperative Preparation and Planning
- Postoperative Hospitalization and First Weeks
- Pectus Bar Removal and Long-Term Results
- What happens if shoemaker’s chest is left untreated?
- Psychological Effects and Loss of Self-Confidence
- Risks of Heart Compression and Respiratory Failure
- Frequently Asked Questions
- Is shoemaker’s chest dangerous?
- How does the shoemaker cross the chest?
- How old is a shoemaker’s chest?
- What does 1 grade of shoemaker’s chest mean?
- Can shoemaker’s chest be corrected with sports?
Shoemaker’s chest is a deformity that occurs when the breastbone collapses inward, which can put pressure on the heart and lungs, and is treated with surgery or vacuum.
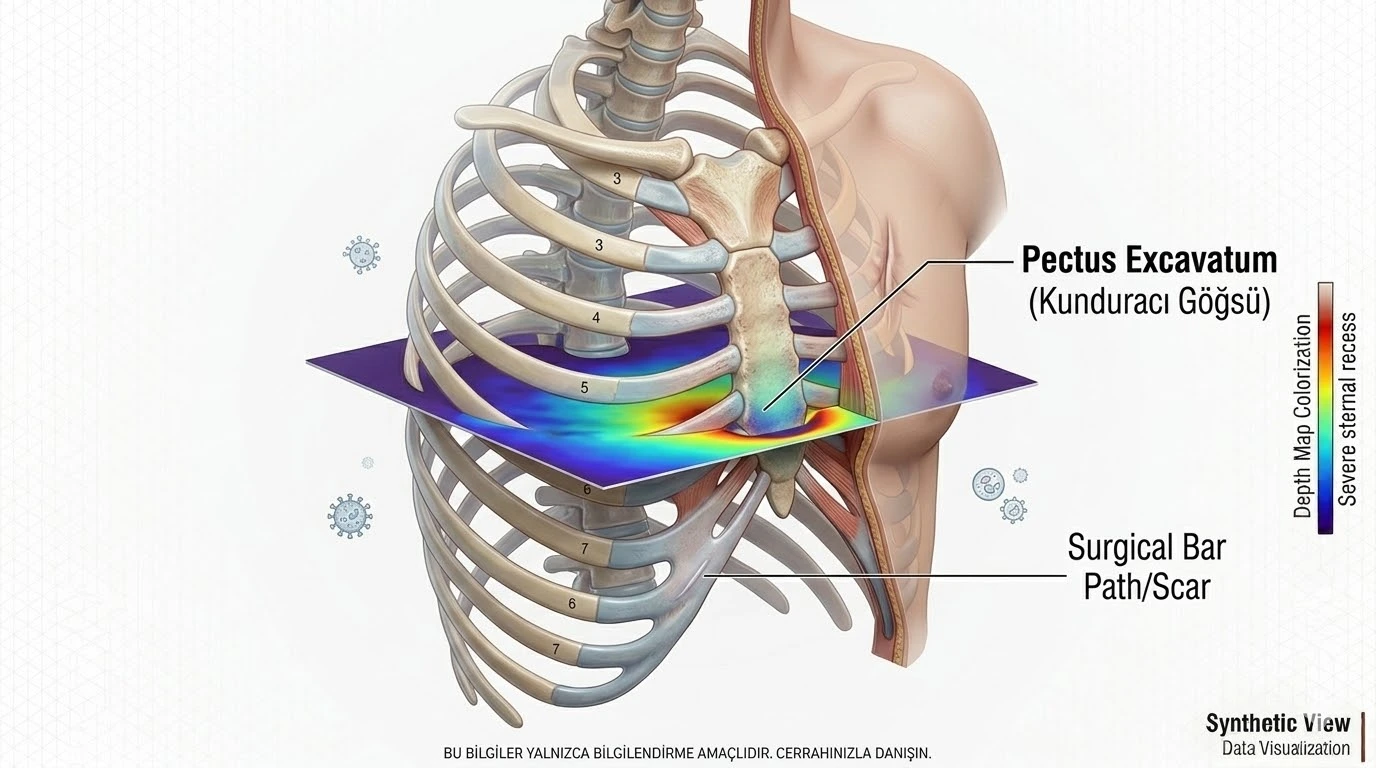
Shoemaker’s chest, known as Pectus Excavatum in the medical literature, is the most common chest wall deformity characterized by the inward collapse of the sternum bone, known as the sternum.
This condition is usually present at birth or becomes evident during the rapid growth spurt of adolescence.
This structural defect in the rib cage is not only an aesthetic concern but also a functional health problem due to the pressure it creates on the heart and lungs.
Thanks to modern medical facilities, today this deformity can be treated with high success rates with both surgical and non-surgical methods.
What is Shoemaker’s Chest (Pectus Excavatum)?
Pectus excavatum is a condition in which the breastbone is pushed towards the spine as a result of the excessive growth of the rib cartilages that form the anterior chest wall.
The reason why it is called “shoemaker’s chest” among the people is the false belief that the tools that shoemakers put on their chests while sewing shoes in the past caused collapse in this area over time.
In reality, this is the result of a purely biological and developmental process.
Causes of Disease and Genetic Factors
Although the exact cause of the disease is not fully known, the irregular development of cartilage tissue is considered the main factor.
In about 40% of cases, there is a family history, which proves that there is a genetic predisposition.
It also has a higher incidence with connective tissue diseases such as Marfan Syndrome or Ehlers-Danlos.
Shoemaker’s Chest Symptoms and Physical Effects
Symptoms vary from patient to patient depending on the depth of the deformity.
While most patients do not feel any complaints other than a hollow in the chest, the following symptoms are observed in severe cases:
- Fatigue and shortness of breath.
- Chest pain and heart palpitations.
- Significant decrease in exercise capacity.
- Posture disorder (shoulders drooping forward).
Diagnostic Methods of Pectus Excavatum
For the right treatment plan, the severity of the deformity and its impact on internal organs must be clearly determined.
Physical Examination and Grading (Haller Index)
The most critical stage of the diagnostic process is measuring the depth of the rib cage.
In Computed Tomography (CT) sections, the “Haller Index” is obtained by dividing the widest transverse diameter of the chest cavity by the narrowest distance between the spine and the breastbone.
While this value is around 2.5 in a normal breast structure, values above 3.25 are classified as “severe deformity” requiring surgical intervention.
Radiological Imaging: CT, MRI, and Echo Tests
While CT scans show the bone structure clearly, MRI (Magnetic Resonance) may be preferred especially in pediatric patients because it does not contain radiation.
Echocardiography (Echo) is used to check whether the collapse is putting pressure (compression) on the right ventricle of the heart.
Evaluation of Heart and Lung Function
Pulmonary function tests (PFT) measure the restriction in lung capacity.
With stress ECG tests, it is analyzed how much strain the patient’s heart is on while moving.
Shoemaker’s Chest Non-Surgical Treatment Methods
In cases that are diagnosed early and not very deep, recovery can be achieved without the need for surgery.
Vacuum Bell (Vacuum Therapy) Application
A Vacuum Bell is a cup-shaped device that is placed on the breastbone and sucks in the air inside, pulling the bone outward.
Especially in childhood and early adolescence, when the bone structure is still flexible, the rib cage can be permanently corrected by using it for a few hours a day.
Chest Wall Exercises and Physiotherapy Support
Although exercises alone do not relieve collapse, they improve posture and strengthen the chest muscles, reducing the visibility of the deformity.
Physiotherapy also plays a major role in the preparation for surgery or recovery process after surgery.
Prof. Dr. Levent Alpay: “Timing is everything in the treatment of shoemaker’s chest. Non-surgical methods such as Vacuum Bell have the highest chance of success between the ages of 12-15. When you notice this situation in your child, instead of waiting for ‘it will go away in time’, getting an expert opinion before the bone structure hardens will make the process much easier.”
Shoemaker’s Chest Surgery (Surgical Treatment)
If the deformity suppresses the internal organs or causes serious psychological trauma to the patient, surgical intervention is inevitable.
Nuss Surgery (Closed Surgical Method)
It is the most commonly applied minimally invasive (closed) method today.
A specially shaped steel or titanium bar is inserted under the breastbone through small incisions made on both sides of the chest.
This bar pushes out the breastbone and usually stays inside for 2-3 years until the bone takes its new form.
Ravitch Surgery (Open Surgical Method)
It is the traditional method preferred in more complicated or asymmetrical cases.
Abnormally developing rib cartilages are removed and the sternum is corrected and fixed.
Although it requires a wider incision than the Nuss method, it is the most reliable way in very hardened rib cages.
The Most Suitable Age Range for Surgical Intervention
The ideal age for surgery is usually between the ages of 13-17.
During this period, the rib cage is flexible enough to take shape and the results are more permanent after correction.
However, successful operations are also performed in adulthood.
Treatment Options Comparison Table
| Feature | Vacuum Bell (Non-Surgical) | Nuss Surgery (Closed) | Ravitch Surgery (Open) |
| Application Time | 6-24 Months (Daily Use) | 60-90 Minutes (Surgical) | 2-3 Hours (Surgical) |
| Hospitalization | None | 4-5 Days | 5-7 Days |
| Incision Scar | None | Very Small (Side) | Medium (Front) |
| Success Rate | High in Mild Case | Very High in Severe Case | High in Complex Case |
| Age Limit | Child/Adolescence Ideal | Over 12 Years Old | Any Age (If Mandatory) |
Surgery Process and Recovery Period
The surgical process is completed with careful planning and subsequent rehabilitation.
Preoperative Preparation and Planning
Before Nuss surgery, the patient is checked for metal allergy (nickel test).
If there are allergies, titanium bars are preferred, preventing the risk of complications.
Postoperative Hospitalization and First Weeks
An epidural catheter or intravenous controlled analgesia is used for postoperative pain management.
Avoiding heavy exercise and impacts for the first month is critical to prevent the bar from moving.
Pectus Bar Removal and Long-Term Results
The inserted bars are removed with a simple procedure after the bone structure stabilizes (usually 2-3 years).
After the bars are removed, the recurrence rate is very low and patients return to a completely normal life.
What happens if shoemaker’s chest is left untreated?
Severe cases of untreated pectus excavatum can lead to more pronounced problems with age.
Psychological Effects and Loss of Self-Confidence
Especially during adolescence, individuals who are ashamed of their breast structure may withdraw from social life and avoid swimming in the sea or wearing tight clothes.
This can result in persistent lack of self-confidence and depression.
Risks of Heart Compression and Respiratory Failure
Pressure from the breastbone on the heart can prevent the heart from pumping blood at full capacity (risks such as mitral valve prolapse).
In addition, since the expansion of the lungs is restricted, chronic fatigue and early respiratory failure can be seen in later ages.
Clinical Experiences and Anonymous Case Examples
Case P: Nuss surgery was performed on a 16-year-old male patient with a Haller Index of 3.8 who had shortness of breath while doing sports.
After the operation, the collapse in the rib cage immediately improved.
Our patient, whose bar was removed 2 years after the operation, is now doing sports at a professional level and does not experience any shortness of breath.
Case V: Vacuum Bell treatment was started in an 11-year-old patient with an incipient deformity.
After 1 year of regular use, the sternum reached its normal position and the treatment was completed without the need for surgery.
Shoemaker’s chest treatment should be customized according to the patient’s age and the severity of the deformity.
You can seek expert opinion to evaluate your or your child’s condition and determine the most appropriate treatment path.
You can have a detailed analysis by making an appointment with our clinic.
Frequently Asked Questions
Is shoemaker’s chest dangerous?
Pectus excavatum is usually not directly life-threatening; However, as the degree of collapse progresses, it can put pressure on the heart and lungs, leading to shortness of breath, fatigue and rhythm disturbances. In addition, it is considered risky in terms of causing serious psychological trauma and lack of self-confidence, especially due to the aesthetic anxiety it creates in young individuals.
How does the shoemaker cross the chest?
Since this condition is an anatomical disorder involving the bone and cartilage structure, it does not go away on its own. Treatment is carried out by a specialist thoracic surgeon with non-surgical methods such as Vacuum Bell (vacuum therapy) or surgical interventions such as Nuss/Ravitch operations, depending on the age of the patient and the severity of the condition.
How old is a shoemaker’s chest?
It is mostly a congenital condition; however, it may not be noticed in infancy. The deformity usually becomes evident during the rapid growth spurt in adolescence (11-15 years) and becomes more deep.
What does 1 grade of shoemaker’s chest mean?
The expression “1st degree” usually means that the deformity is mild, the collapse in the rib cage is not very deep and does not put any meaningful pressure on the internal organs (heart, lungs). Patients at this level are usually followed up clinically or monitored with physical therapy/vacuum methods.
Can shoemaker’s chest be corrected with sports?
Sports and special chest exercises do not completely eliminate bone collapse in the rib cage. However, developing the chest muscles and correcting posture disorders makes the hollow less noticeable when viewed from the outside and increases the patient’s condition.
Scientific Bibliography
- PubMed: Long-term results of the Nuss procedure
- The Lancet: Pectus excavatum: from diagnosis to therapy
- Journal of Pediatric Surgery: Vacuum bell treatment of pectus excavatum
