Ingredients
- What is Myasthenia Gravis? Why Does It Happen?
- Myasthenia Gravis Symptoms and Clinical Findings
- Weakness in the Eye and Facial Muscles (Ocular Myasthenia)
- Chewing, Swallowing and Speech Disorders
- Myasthenic Crisis: Risk of Respiratory Failure
- The Relationship Between Myasthenia Gravis and the Thymus Gland
- Thymic Hyperplasia and Thymoma Presence
- Myasthenia Gravis Diagnosis and Diagnostic Methods
- Edrophonium (Tensilon) Test and Antibody Tests
- Electromyography (EMG) and Radiological Imaging
- Myasthenia Gravis Treatment Options
- Drug Treatments and Plasmapheresis Applications
- Surgical Intervention in Myasthenia Gravis: Thymectomy
- Which Patients Is Thymectomy Surgery Applied To?
- Closed Thymectomy Methods (VATS and Robotic Surgery)
- Effects of Surgery on Neurological Recovery
- Preoperative Preparation and Postoperative Follow-up Process
- Frequently Asked Questions
- Can Medications Be Completely Discontinued After Thymectomy Surgery?
- Should Every Myasthenia Gravis Patient Have Surgery?
- What is the Success Rate of the Surgery and When Does It Take Effect?
Myasthenia Gravis is a chronic and autoimmune neuromuscular disease that occurs as a result of impaired communication between the nervous system and muscles.
The disease is characterized by the body’s immune system producing faulty antibodies against its own tissues.
This picture, which means “severe muscle weakness” in the medical literature, manifests itself as fatigue and weakness, especially in the muscles we control voluntarily.
Today, Myasthenia Gravis is a disease that can be successfully managed with the joint work of neurological drug treatments and thoracic surgery (thymectomy) disciplines.
Early diagnosis and correct surgical intervention can improve patients’ quality of life and provide long-term complete recovery (remission).
What is Myasthenia Gravis? Why Does It Happen?
For a normal muscle contraction, a substance called acetylcholine, released from nerve endings, must bind to receptors (receptors) on the muscle.
In patients with Myasthenia Gravis, the immune system produces abnormal antibodies that target these receptors.
These antibodies invade or destroy the areas where acetylcholine will bind, preventing the “move” command from the nerve from reaching the muscle.
Although it is not known exactly why the disease develops in some individuals, it has been proven that the thymus gland, located in the chest cavity, plays a central role in the production of this faulty antibody.
The disease can be seen at any age; However, it is usually more commonly diagnosed in young women (20-30 years) and older men (over 60 years).
Myasthenia Gravis Symptoms and Clinical Findings
The most characteristic feature of Myasthenia Gravis is that muscle weakness improves with rest and increases with movement or later in the day.
Symptoms may differ from person to person and may progress as attacks (flare-ups) that vary in severity over time.
Weakness in the Eye and Facial Muscles (Ocular Myasthenia)
In more than 50% of patients, the first symptoms appear in the eye muscles and this picture is called “Ocular Myasthenia”.
- Droopy Eyelid (Ptosis): It usually starts unilaterally, becomes evident towards the end of the day and may restrict the patient’s field of vision.
- Double Vision (Diplopia): It occurs as a result of the incompatible functioning of the muscles that move the eyes.
- Change in Facial Expression: Due to weakness in the facial muscles, a “growling”-like expression may occur during smiling or facial expressions may become dull.
Chewing, Swallowing and Speech Disorders
When the disease affects the muscles of the face and throat, basic functions in daily life begin to become difficult.
- Speech Change: Speech gradually begins to come from the nose (nasal speech) or the words roll in the mouth.
- Difficulty Swallowing: Fatigue while eating, food getting into the throat or fluids coming back up through the nose may occur.
- Fatigue in Chewing Muscles: When chewing hard foods, the jaw muscles quickly become tired and the patient may have to stop eating halfway.
Myasthenic Crisis: Risk of Respiratory Failure
The most feared picture of Myasthenia Gravis that requires urgent intervention is the “Myasthenic Crisis”.
In this case, the respiratory muscles (diaphragm and intercostal muscles) become too weak to continue breathing.
Infections, stress, side effects of certain medications, or inadequate treatment can trigger this crisis.
When the patient starts to suffer from shortness of breath, he should be treated in intensive care conditions without delay and respiratory support should be provided.
The Relationship Between Myasthenia Gravis and the Thymus Gland
The thymus gland is an organ located in the center of the chest cavity and is considered the “training center” of the immune system.
Scientific research shows that in patients with Myasthenia Gravis, the thymus gland produces erroneous signals that command the immune system to “attack its own receptors”.
Therefore, surgical removal of the thymus gland (thymectomy) is one of the most effective steps towards drying out the source of the disease.
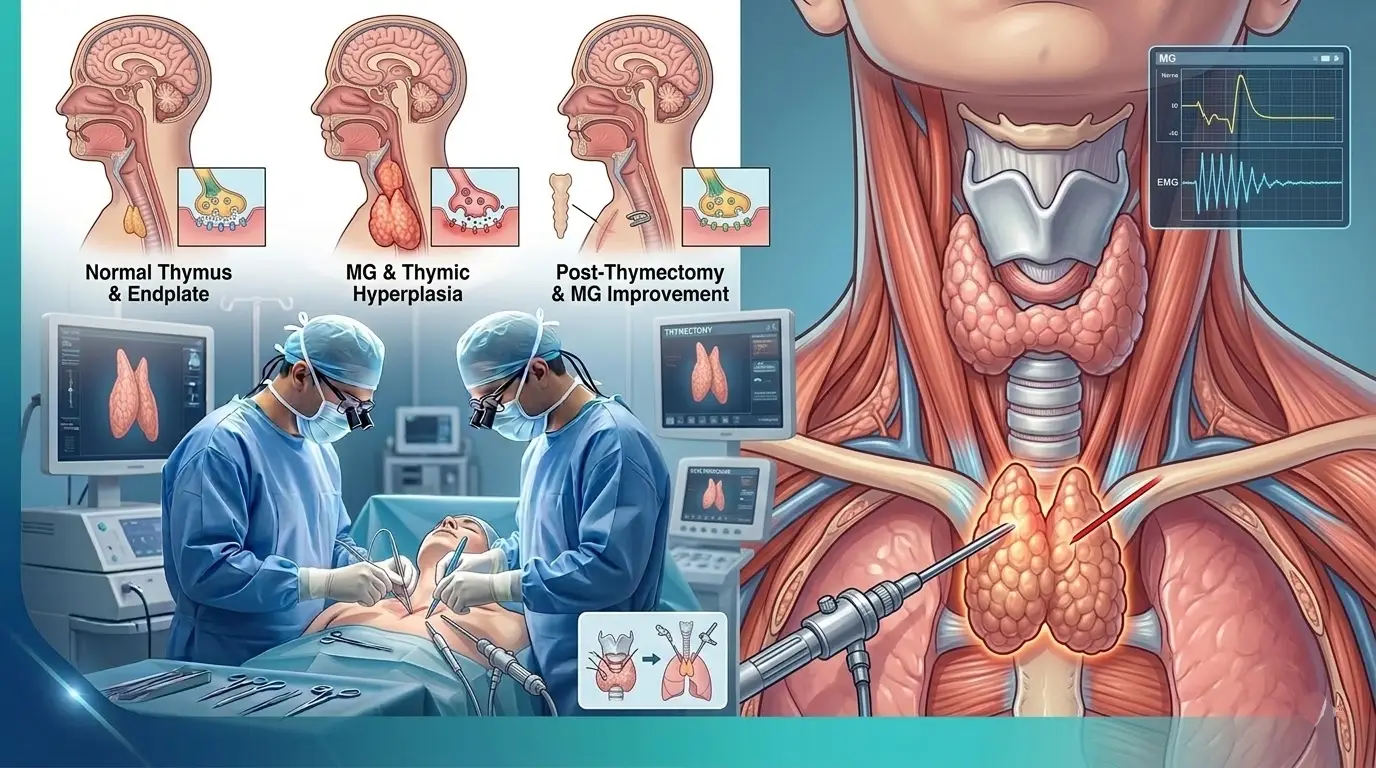
Thymic Hyperplasia and Thymoma Presence
In the vast majority of patients diagnosed with Myasthenia Gravis, abnormalities are detected in the thymus gland.
- Thymic Hyperplasia: The thymus gland is more active and larger than normal. This picture is observed in approximately 70% of MG patients.
- Thymoma: They are tumors that develop on the thymus gland. Thymoma is detected in approximately 15% of MG patients and these tumors must be surgically removed.
Prof. Dr. Levent Alpay: One of the first things to be done in every patient diagnosed with Myasthenia Gravis is to examine the thymus gland with a high-resolution chest tomography. If there is a growth or tumor (thymoma) in the thymus, the surgical option is no longer a choice but becomes the cornerstone of treatment. With surgery, we not only remove the tumor, but also aim to reduce the patient’s neurological dependence on medication.
Myasthenia Gravis Diagnosis and Diagnostic Methods
The diagnosis of Myasthenia Gravis (MG) is made by combining the patient’s clinical history with specific neurological and radiological tests.
In the diagnostic process, the main goal is to prove that the muscle weakness is caused by a conduction disorder at the nerve-muscle junction.
Edrophonium (Tensilon) Test and Antibody Tests
The edrophonium test is the observation of a sudden increase in muscle strength by administering a short-acting drug intravenously to the patient; however, it is rarely applied today due to its side effects.
One of the most reliable methods in diagnosis is to measure the level of “Acetylcholine Receptor Antibodies” (AChR) with a blood test.
In the vast majority of patients, these antibodies are positive; In negative cases, rarer antibodies such as “MuSK” are investigated.
Electromyography (EMG) and Radiological Imaging
In the EMG test, low-dose electrical impulses given to the muscles clearly reveal the fatigue (discharge) in conduction.
Radiological imaging determines the surgical dimension of the work; Chest Tomography (CT) should be performed on every MG patient to see if there is a tumor (Thymoma) in the thymus gland.
Myasthenia Gravis Treatment Options
MG treatment is a long-term process based on controlling symptoms and suppressing the immune system.
Drug Treatments and Plasmapheresis Applications
In first-line treatment, pyridostigmine-based drugs that increase nerve-muscle conduction are usually used.
Cortisone or other immunosuppressive drugs may be added to the treatment to suppress the immune system.
During periods when the disease is severe or preoperative preparation is required, “Plasmapheresis” or “IVIG” (Intravenous Immunoglobulin) methods are used to clear harmful antibodies from the blood.
Surgical Intervention in Myasthenia Gravis: Thymectomy
Thymectomy is the surgical complete removal of the thymus gland in the center of the rib cage.
This surgery aims to permanently change the course of the disease by eliminating the faulty production center of the immune system.
Which Patients Is Thymectomy Surgery Applied To?
Surgery is mandatory in all MG patients with a tumor (Thymoma) in the thymus gland.
Even if there is no tumor, it has been scientifically proven that surgery provides great benefits in patients with diffuse MG under the age of 65 and with antibody positivity.
Thymectomy performed early in the disease (within the first 1-2 years) maximizes the chances of recovery.
Closed Thymectomy Methods (VATS and Robotic Surgery)
Today, complete cleaning, which we call “maximal thymectomy”, is successfully performed with closed methods (VATS or Robotic) instead of large incisions.
These surgeries, which are performed through small holes, preserve the patient’s breathing capacity and minimize the risk of infection.
MG Treatment Methods Comparison Table
| Method | Mechanism of Action | Application Purpose | Recovery Prospect |
| Medication | Increases transmission / Suppresses immunity | Symptom control | Temporary and permanent use |
| Closed Thymectomy | Removes antibody production center | Permanent improvement (Remission) | Long-term and permanent |
| Plasmapheresis | Clears existing antibodies | Emergency/Crisis management | Fast but short-term |
Effects of Surgery on Neurological Recovery
The effect of thymectomy surgery is usually not seen the next day; It may take months or even years for the immune system to reorganize.
The following healing processes are usually observed in patients:
- Significant reduction of drug doses.
- In some patients, complete cessation of drugs (Complete remission).
- Significant reduction in the frequency and severity of attacks.
Preoperative Preparation and Postoperative Follow-up Process
The surgical process for MG patients requires full compliance of neurology and thoracic surgery.
Before surgery, the patient’s clinical condition is stabilized; muscle strength is supported by IVIG or plasmapheresis if necessary.
Thanks to closed methods after surgery, the patient is discharged in 2-3 days, but the follow-up of neurological drugs is carried out meticulously.
Prof. Dr. Levent Alpay: Myasthenia Gravis surgery is not a simple “organ removal” procedure. The surgeon needs to remove all fat tissues around the thymus gland to the millimeter (maximal resection). Because even a small thymus tissue left behind can continue to produce faulty antibodies. This sensitivity directly determines the neurological benefit the patient will receive from surgery.
Case Experience (Anonymous):
Robotic thymectomy was performed in a 28-year-old patient who frequently experienced difficulty in swallowing and droopy eyelids despite drug treatment, in the 8th month of his illness. In the 1st year after the surgery, our patient’s drug doses were reduced by half and he was able to do his daily activities without any restrictions.
To get more information about Myasthenia Gravis surgery or to evaluate your condition, you can make an appointment with our clinic and seek expert opinion.
Frequently Asked Questions
Can Medications Be Completely Discontinued After Thymectomy Surgery?
In approximately 30-40% of patients, drugs can be completely discontinued; In the remaining patients, a significant decrease in drug doses and symptom relief is achieved.
Should Every Myasthenia Gravis Patient Have Surgery?
If thymoma is present, surgery is essential. If there is no thymoma, the patient’s age, antibody status and duration of the disease are evaluated and the decision for surgery is made individually.
What is the Success Rate of the Surgery and When Does It Take Effect?
The positive effects of thymectomy are usually most pronounced between the 6th month and 2nd year after surgery. The success rate is higher in the early stages.
Scientific Bibliography
- New England Journal of Medicine (NEJM): Thymectomy Trial in Non-Thymomatous Myasthenia Gravis
- Neurology: Practice guideline update summary: Thymectomy in Myasthenia Gravis
- PubMed: Long-term results of robotic thymectomy for Myasthenia Gravis
- The Lancet Neurology: Current treatments and future perspectives in MG
