Ingredients
- What is Diaphragm Paralysis? Why Does It Happen?
- Main Respiratory Muscle: The Function of the Diaphragm
- Unilateral and Bilateral (Bilateral) Diaphragm Paralysis
- Causes and Risk Factors of Diaphragm Paralysis
- Phrenic Nerve Injury and Traumas
- Postoperative Diaphragmatic Paralysis
- What are the Symptoms of Diaphragm Paralysis?
- Shortness of Breath Increasing When Lying Down (Orthopnea)
- Fatigue During Exertion and Respiratory Distress
- Diaphragmatic Paralysis Diagnosis and Diagnostic Methods
- Movement Analysis with Fluoroscopy (Sniff Test)
- Pulmonary Function Tests (PFT) and Electromyography (EMG)
- Diaphragm Paralysis Treatment Options
- Surgical Treatment: Diaphragm Pilation (Stretching Surgery)
- Robotic and Closed (VATS) Diaphragm Surgery
- Frequently Asked Questions
- Does Diaphragm Paralysis Go Away on Its Own?
- Is Diaphragm Surgery Risky?
- Who is Diaphragm Battery (Pacemaker) Applied to?
Diaphragm paralysis is a condition in which the diaphragm, which is the most basic respiratory muscle that separates the chest cavity and the abdominal cavity, loses its function.
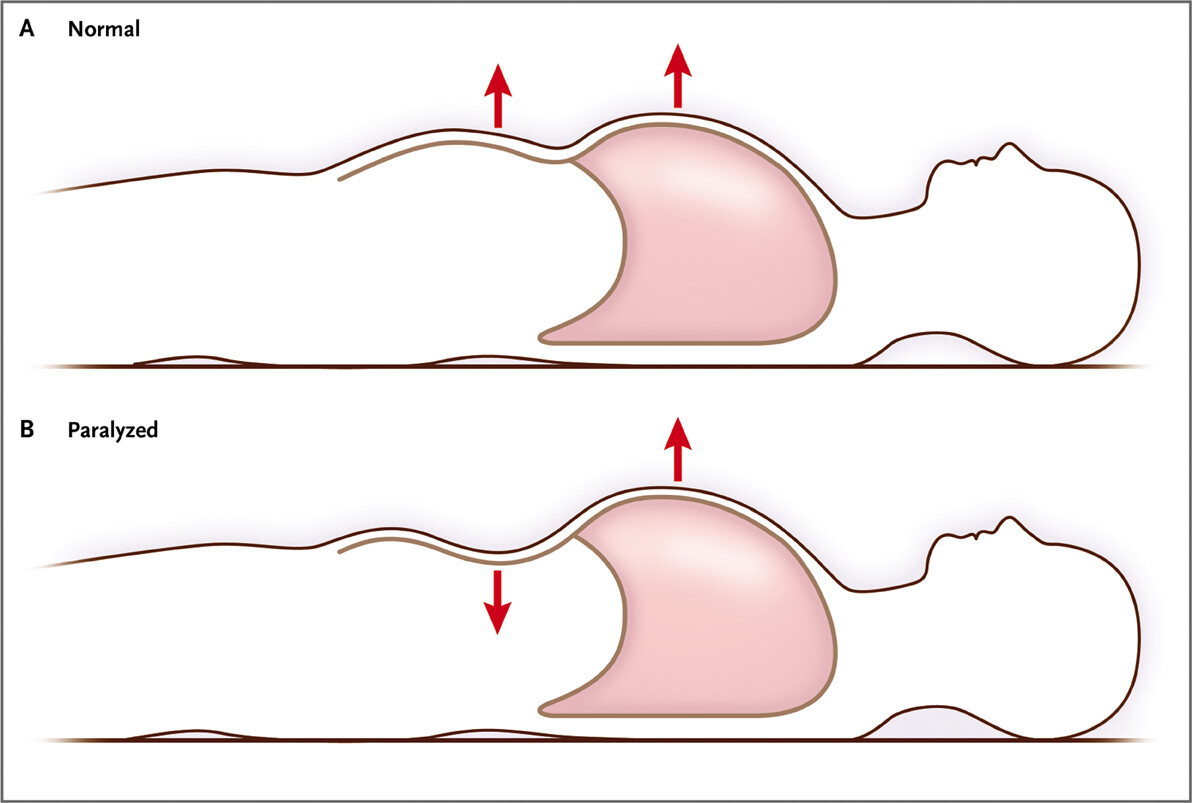
Under normal conditions, when we breathe, the diaphragm contracts and descends, creating space for the lungs to fill with air; However, in the event of a stroke, this muscle cannot move.
The failure of the diaphragm to function leads to a significant decrease in lung capacity and severe shortness of breath, which reduces the patient’s quality of life.
This condition, which is usually unilateral, can rarely affect both diaphragm muscles and become severe enough to make the patient dependent on a ventilator.
Modern thoracic surgery techniques make it possible to open up breathing space for the lungs by re-tightening the dysfunctional and relaxed diaphragm muscle.
What is Diaphragm Paralysis? Why Does It Happen?
Diaphragmatic paralysis occurs as a result of interruption of the conduction of the phrenic nerve, which provides the movement of this muscle, or direct damage to muscle tissue.
The paralyzed diaphragm muscle loses its normal tense and dome-like structure, relaxes and is pushed upwards into the chest cavity by the pressure of the intra-abdominal organs.
This elevation causes the lung on that side to deflate and fail to expand sufficiently during breathing.
Main Respiratory Muscle: The Function of the Diaphragm
The diaphragm is like the main engine of our body and involuntarily contracts thousands of times a day to perform breathing.
During inhalation, it creates a vacuum effect, drawing air into the lungs, and during exhalation, it relaxes and allows carbon dioxide to be expelled.
Paralysis of this muscle causes the respiratory load to be placed only on the intercostal muscles, which causes the body to tire quickly.
Unilateral and Bilateral (Bilateral) Diaphragm Paralysis
Diaphragmatic paralysis presents with two different clinical pictures depending on the extent of involvement.
- Unilateral Paralysis: Usually only one of the right or left diaphragm is affected; While patients do not have problems at rest, they become blocked when they exert effort.
- Bilateral Paralysis: It occurs when the phrenic nerve on both sides is damaged; This is a very severe respiratory failure that requires urgent medical attention.
Unilateral paralysis is more common and is often detected incidentally on chest X-rays taken while investigating another disease.
Causes and Risk Factors of Diaphragm Paralysis
The causes of paralysis of the diaphragm are very diverse and can sometimes be the first harbinger of another underlying disease.
Phrenic Nerve Injury and Traumas
The phrenic nerve, which carries the movement order of the diaphragm, leaves the neck region, passes past the heart and reaches the diaphragm; It can be damaged at any point along this long route.
Neck hernias, tumor compressions or severe blows to the neck area can interrupt nerve conduction and lead to paralysis.
Additionally, trauma that shakes the rib cage, such as traffic accidents or falling from a height, can also damage the nerve structure of the diaphragm.
Postoperative Diaphragmatic Paralysis
Especially after heart and lung surgeries, temporary or permanent paralysis of the phrenic nerve can be seen due to the surgical procedure or cold application (ice water).
This condition is usually noticed after surgery when the patient breathes more difficult than expected or cannot leave the ventilator.
Some viral infections and neurological diseases (e.g. ALS or MS) can also trigger diaphragm paralysis by causing nerve damage.
What are the Symptoms of Diaphragm Paralysis?
Symptoms vary depending on whether the paralysis is unilateral or bilateral and the patient’s current lung capacity.
Shortness of Breath Increasing When Lying Down (Orthopnea)
The most typical symptom of diaphragmatic paralysis is that the patient stops breathing when lying flat.
When the patient lies down, the intra-abdominal organs slide upwards with the effect of gravity and push the already loose diaphragm towards the lung.
For this reason, patients usually prefer to sleep with a high pillow or complain that they feel pressure in their breasts when they lie down.
Fatigue During Exertion and Respiratory Distress
A healthy person uses their diaphragm more actively when climbing hills or climbing stairs; However, the paralyzed patient does not have this capacity.
Palpitations, fatigue and the feeling of “I can’t breathe” that occur even in simple daily activities are classic findings of diaphragm paralysis.
Diaphragmatic Paralysis Diagnosis and Diagnostic Methods
The diagnostic process is clarified by tests based on monitoring the movement of the diaphragm live, rather than a physical examination.
Movement Analysis with Fluoroscopy (Sniff Test)
The gold standard in diagnosis is the fluoroscopic examination known as the “Sniff Test” (sniff test).
Under radiology, the patient is asked to breathe quickly through his nose; The diaphragm, which should normally go down, shoots upwards (paradoxical movement) if it is paralyzed.
This test definitively shows whether the diaphragm is just at rest or is working in the opposite direction.
Pulmonary Function Tests (PFT) and Electromyography (EMG)
Pulmonary function tests measure the patient’s capacity while sitting and lying down; A decrease in capacity of more than 20% while lying down is in favor of paralysis.
EMG (nerve measurement), on the other hand, is used to assess the electrical activity of the phrenic nerve to determine the extent of damage and the potential for healing.
Diaphragm Paralysis Treatment Options
Not all diaphragmatic paralysis requires surgery; However, if the patient’s shortness of breath interferes with his daily life, surgical solution is the most effective way.
Surgical Treatment: Diaphragm Pilation (Stretching Surgery)
Pilation surgery is the process of folding and tightening the loosened and ballooning diaphragm muscle with special sutures.
In this way, the diaphragm is pulled down, the chest cavity expands and the deflated lung tissue can be filled with air again and expand.
Since the tense diaphragm muscle can no longer run up, other healthy respiratory muscles begin to work more efficiently.
Robotic and Closed (VATS) Diaphragm Surgery
Today, we can now perform diaphragm surgeries with closed methods (thoracoscopic or robotic) without making large incisions.
In this procedure, which is performed through small holes, blood loss is minimal and the patient’s recovery rate is much higher than open surgery.
Closed surgery provides a great advantage, especially for these patients with limited respiratory capacity, due to the low postoperative pain.
Treatment Options and Expectations Table
| Feature | Observation and Follow-up | Diaphragm Piling (Surgery) |
| To Whom Is It Applied? | Asymptomatic / Mild cases | Those with severe shortness of breath |
| Method | Breathing exercises | Closed or Robotic Surgery |
| Hospital Stay | Not required | 2 – 3 Days |
| Improvement in Breathing | Restricted | Distinct and Permanent |
| Recovery Time | The process is uncertain | 2 – 4 Weeks |
Prof. Dr. Levent Alpay: Patients with diaphragmatic paralysis can often waste time in the wrong branches by saying “Is there a problem with my heart?” or “Do I have asthma?”. If your shortness of breath becomes evident only when you lie flat, you should definitely see a thoracic surgeon and have your diaphragm movements checked. Early pilation surgery can bring your deflated lung back to life and give you a deep breath.
Case Experience (Anonymous):
A 58-year-old patient presented with complaints of panting while climbing a hill and not being able to lie flat at night after a viral infection. In the Sniff test, it was seen that his left diaphragm was completely paralyzed and he went up and deflated his lung by 40%. After the diaphragm pilation we performed with the robotic method, our patient’s lung was completely opened and he started to sleep comfortably without using a high pillow only 2 weeks after the operation.
If you experience increased shortness of breath or an unexplained decrease in your effort capacity while lying down, you can make an appointment with our clinic and seek expert opinion for a detailed evaluation of your diaphragm functions.
Frequently Asked Questions
Does Diaphragm Paralysis Go Away on Its Own?
If the paralysis is caused by exposure to cold or a temporary inflammatory condition, it may resolve spontaneously within 6-12 months; however, in traumatic or surgical damage, it is likely to be permanent.
Is Diaphragm Surgery Risky?
Every surgical procedure has risks; However, diaphragm pilation performed with modern closed methods is a procedure with a very low complication rate and a high chance of success.
Who is Diaphragm Battery (Pacemaker) Applied to?
Diaphragm pacemaker is a special method preferred to stimulate the nerve, usually in patients who are paralyzed on both sides due to cervical spinal cord injury and live on a ventilator.
Scientific Bibliography
- The Society of Thoracic Surgeons: Surgical Plication for Diaphragm Paralysis
- Journal of Thoracic and Cardiovascular Surgery: Minimally Invasive Diaphragm Plication
- PubMed (NCBI): Etiology and Pathophysiology of Diaphragmatic Paralysis
- Cleveland Clinic: Diaphragm Paralysis Diagnosis and Management
