
Ingredients
- Trachea Surgery and Airway Diseases
- What is Tracheal Stenosis? Why Does It Happen?
- Tracheal Tumors: Benign and Malignant Masses
- Strictures After Intubation and Tracheostomy
- Esophageal Diseases and Surgical Treatment
- Esophageal Cancer and Modern Surgical Approaches
- Esophageal Strictures and Diverticula (Zenker’s Diverticulum)
- Achalasia and Gastric Hernia (Reflux) Surgery
- Common Problems Between the Trachea and Esophagus
- Tracheo-esophageal Fistulas (TEF): Symptoms and Treatment
- Diagnosis and Diagnostic Methods: Endoscopy and Bronchoscopy
- Advanced Surgical Techniques in Airway and Esophagus
- Tracheal Resection and End-to-End Anastomosis (Gold Standard)
- Closed Esophageal Surgeries (VATS and Robotic Surgery)
- Stent Applications and Endoscopic Expansion (Dilation)
- Post-Operative Care and Quality of Life
- Frequently Asked Questions
- Is Hoarseness Permanent After Tracheal Surgery?
- How Should Nutrition Be After Esophageal Surgery?
- Do Airway Stenosis Recur?
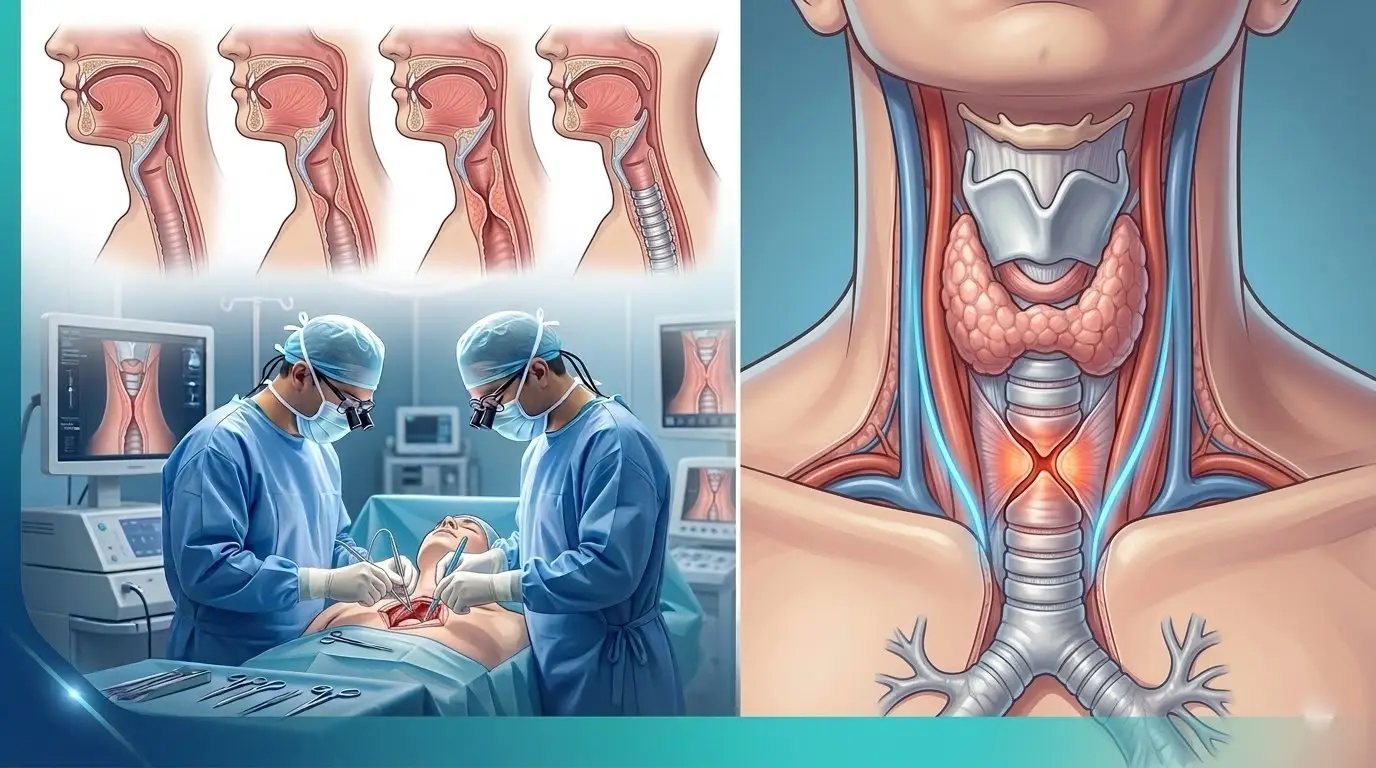
Airway and esophageal surgery is a surgical field that requires high technical skills, covering the diseases of the two critical channels that provide breathing and nutrition, which are the most basic vital functions of the body.
The trachea carries air to the lungs, while the esophagus (esophagus) delivers food to the stomach; These two structures are anatomically adjacent to each other and are commonly affected by many diseases.
Strictures, tumors or injuries in this area are conditions that seriously threaten the patient’s quality of life and may require urgent intervention.
Today, this surgical discipline aims to restore the integrity of these ducts through both open and closed (VATS/Robotic) methods.
Accurate diagnosis and timely surgical intervention ensure that the patient can both breathe comfortably and feed unhindered.
Trachea Surgery and Airway Diseases
Tracheal surgery treats functional and structural disorders of the tubular structure, which starts under the larynx and extends to the main bronchi branching into the lungs.
Keeping the airway open is a vital necessity; Even the slightest narrowing of this canal creates severe shortness of breath and a feeling of suffocation in the patient.
What is Tracheal Stenosis? Why Does It Happen?
Tracheal stenosis is a condition in which the inner diameter of the trachea narrows for various reasons, restricting airflow.
The most common causes include long-term intensive care hospitalizations, traumas, caustic substance ingestion and rarely congenital anomalies.
As the stenosis progresses, the patient experiences a whistling-like breathing (stridor) and increased breathing hunger with exertion.
Tracheal Tumors: Benign and Malignant Masses
Although tracheal tumors are rare, they usually show symptoms with coughing up blood or shortness of breath.
Malignant types such as squamous cell carcinoma (SCC) or adenoid cystic carcinoma are often encountered, while benign masses such as papillomas can also be seen.
The location and extent of the tumor is the most important criterion in determining the surgical technique.
Strictures After Intubation and Tracheostomy
In patients who are connected to a ventilator in intensive care, the bubble of the tube (intubation tube) placed in the trachea can put pressure on the trachea wall and disrupt blood flow.
As this condition heals, a hard scar tissue (scar) forms in the area and the trachea narrows; A similar situation may develop after a hole in the throat (tracheostomy).
These patients usually begin to experience shortness of breath weeks after weaning from the device, and it is critical not to confuse this condition with asthma.
Esophageal Diseases and Surgical Treatment
Esophageal surgery covers a wide range from mechanical strictures that prevent food delivery to cancer.
Esophageal Cancer and Modern Surgical Approaches
Esophageal cancer is a disease that manifests itself with difficulty in swallowing and can be completely cured with surgery when caught at an early stage.
Surgical treatment (esophagectomy) involves removing the diseased part of the esophagus and creating a new food tract, usually by pulling the stomach up.
Esophageal Strictures and Diverticula (Zenker’s Diverticulum)
Zenker diverticulum is a pocketing that forms in the upper part of the esophagus, where food accumulated can come back up into the mouth or lead to infection.
Strictures, on the other hand, usually develop after chemical burns or radiotherapy and can make it impossible for the patient to eat solid food.
Achalasia and Gastric Hernia (Reflux) Surgery
Achalasia is a swallowing disorder that occurs as a result of the inability of the muscles at the entrance of the esophagus to the stomach to relax.
In surgical treatment, these muscles are cut with the method called “Heller Myotomy” and the transition is relieved; In cases of hiatal hernia (reflux), repair of the hernia and strengthening of the stomach entrance (Nissen fundoplication) are applied.
Common Problems Between the Trachea and Esophagus
The neighborhood of these two organs sometimes causes the problem in one to spread to the other or to form unwanted connections between them.
Tracheo-esophageal Fistulas (TEF): Symptoms and Treatment
TEP is the formation of an abnormal channel between the trachea and esophagus; In this case, the food eaten and stomach acid escape directly into the lungs.
This condition, which usually develops as a result of cancer progression or trauma, leads to recurrent pneumonia and life-threatening injuries.
Treatment is a complex process that requires surgical closure of this canal and placement of tissue patches in between.
Diagnosis and Diagnostic Methods: Endoscopy and Bronchoscopy
In diseases of the airway and esophagus, “looking from the inside” methods are the cornerstone of diagnosis.
- Bronchoscopy: It is used to examine the inside of the trachea, measure the level of stenosis, and take biopsies if necessary.
- Endoscopy (Gastroscopy): It is the gold standard for assessing the internal structure of the esophagus, the presence of tumors, or contractile disorders.
- CT and MRI: It shows the outer walls of the organs and their relationship with the surrounding tissues in millimeters.
Advanced Surgical Techniques in Airway and Esophagus
Modern thoracic surgery not only opens these channels but also aims to return the patient’s anatomy to its most natural state.
Tracheal Resection and End-to-End Anastomosis (Gold Standard)
It is the process of suturing the intact ends together after removing the tracheal cut with stenosis or tumor.
This method is the permanent and most successful treatment method for tracheal stenosis; When performed in expert hands, it ensures that the patient does not experience shortness of breath again throughout his life.
Closed Esophageal Surgeries (VATS and Robotic Surgery)
Esophageal cancer surgeries are now performed by entering the chest cavity through small holes (VATS or Robotics) instead of large incisions.
Robotic surgery offers superior vision and mobility to the surgeon in cleaning the lymph nodes around the esophagus and connecting sutures with the stomach.
Stent Applications and Endoscopic Expansion (Dilation)
In patients who are not suitable for surgery or require palliative support, stents placed in the stenosis area keep the canal open.
In partial stenosis, the patient’s nutrition can be temporarily provided by dilating with endoscopic balloons.
Treatment Methods Comparison Table
| Feature | Tracheal Resection (Surgery) | Stent Application | Endoscopic Dilation |
| Persistence | High (Permanent solution) | Medium (Replacement may be required) | Low (Requires repetition) |
| Application Area | Structural stenosis / Tumors | Advanced blockages | Simple and elastic stenosis |
| Healing Process | 1 – 2 weeks hospital | Discharge on the same day | Discharge on the same day |
| Success Rate | 90%+ (In the appropriate case) | Symptomatic relief | Temporary relief |
Post-Operative Care and Quality of Life
After these surgeries, patients are asked to pay attention to their neck movements and diet.
After tracheal surgery, it may be necessary to keep the neck tilted forward for a certain period of time to reduce tension in the suture line.
Patients who have had esophageal surgery are accustomed to eating small portions and frequent meals; Over time, the body adapts to this new system.
Prof. Dr. Levent Alpay: Airway and esophageal surgery is a field that does not forgive mistakes. Especially in tracheal stenosis, temporary solutions such as “laser burning” or “balloon dilation” can sometimes cause the stenosis to deepen and make the chance of surgery difficult. For this reason, it is vital that the first intervention is planned by teams that are competent to perform resection, which is a definitive treatment.
Case Experience (Anonymous):
A young patient who was discharged after being in intensive care for a long time and treated with the diagnosis of “asthma” 2 months later applied to our clinic with increasing shortness of breath. Bronchoscopy showed that the trachea was 90% obstructed (subglottic stenosis). After the tracheal resection and end-to-end anastomosis surgery, the patient started to breathe easily on the operating table and was discharged on the 5th day with complete recovery.
If you have complaints of difficulty swallowing or unexplained shortness of breath, you can make an appointment with our clinic for professional management of these complex processes and seek expert opinion.
Frequently Asked Questions
Is Hoarseness Permanent After Tracheal Surgery?
The nerves that control the vocal cords are very close to the trachea; These nerves are preserved during surgery, but there may be short-term hoarseness due to temporary edema, and the risk of permanent damage is very low in experienced hands.
How Should Nutrition Be After Esophageal Surgery?
The first weeks start with liquid and soft foods, over time, as the stomach capacity and the new way adapt, normal foods are started; Small but frequent nutrition is the basic rule.
Do Airway Stenosis Recur?
If the stenosis is completely removed surgically and healthy tissues are combined (resection), the risk of recurrence is minimal; However, recurrence is common after procedures such as stents or balloons.
Scientific Bibliography
- The Journal of Thoracic and Cardiovascular Surgery: Tracheal Resection and Reconstruction: Technical Considerations
- Lancet Oncology: Modern Management of Esophageal Cancer
- PubMed (NCBI): Complications of prolonged intubation: Tracheal stenosis
- Annals of Surgery: Robotic vs. Minimally Invasive Esophagectomy
