
Ingredients
- What is a Tracheal Stent? Why is it applied?
- Tracheal Stenosis (Tracheal Stenosis) and Stent Relationship
- The Role of Stents in Achieving Airway Patency
- In Which Situations Is Tracheal Stent Used?
- Airway Obstructions Due to Malignant Tumors
- Benign Strictures and Tracheomalacia (Tracheal Softening)
- What are the Types of Tracheal Stents?
- Silicone Stents (Dumont Stent) and Their Advantages
- Self-Expanding Metallic Stents (Nitinol Stent)
- Hybrid Stent Designs
- How is a Tracheal Stent Inserted? Application Process
- Stent Placement Under Rigid Bronchoscopy
- Preparation and Anesthesia Before Stent Application
- Advantages of Tracheal Stent Application and Expected Results
- Immediate relief from shortness of breath
- Increased Quality of Life and Effort Capacity
- Post-Stent Care and Follow-up Process
- Stent Cleaning and Moisturizing Recommendations
- Possible Complications: Displacement and Mucus Obstruction
- Frequently Asked Questions
- How Long Can a Tracheal Stent Stay in the Body?
- Is Speech or Swallowing Affected After Stent Placement?
- Can the Inserted Stent Be Removed Later?
- Scientific Bibliography
Tracheal stent applications are a vital medical intervention that allows the mechanical opening of stenosis or collapses in the trachea (trachea).
Since the trachea is the main pipeline that carries air to the lungs, even the slightest narrowing in this area causes a severe feeling of suffocation and respiratory failure in the patient.
Stents are hollow, tubular supporting devices placed in this narrowed area, and their main job is to ensure that the airway remains open continuously.
Today, with the developing technology, the biocompatibility of stents has increased and placement techniques have been modernized to maximize patient comfort.
This procedure is considered the gold standard for patients, especially those who are not eligible for tracheal surgery or require immediate respiratory support.
What is a Tracheal Stent? Why is it applied?
A tracheal stent is a medical prosthesis that supports the internal structure of the trachea and keeps the wall upright against external pressure.
This application is preferred in cases where surgical removal of the narrowing of the trachea is not possible or when the patient needs to be allowed to breathe during the preparation process for surgery.
Stent application is not just a tube placement procedure, it is an operation to restore the patient’s basic life functions.
Tracheal Stenosis (Tracheal Stenosis) and Stent Relationship
Tracheal stenosis develops when the tissue shrinks by forming scars (scars) as a result of being connected to a ventilator for a long time, traumas or tumors.
When this stenosis reaches a critical level, meaning the trachea diameter narrows by more than 50%, stent placement becomes essential.
The stent expands this annular tissue, which has narrowed, allowing air to reach the lungs unhindered.
The Role of Stents in Achieving Airway Patency
Stents act as an endoskeleton, maintaining the structural integrity of the windpipe.
Especially when there is external tumor pressure or when the cartilage structure of the trachea softens, the stent resists this pressure and prevents the tube from collapsing.
In this way, it becomes easier for the patient to cough up sputum and risks such as lung collapse (atelectasis) are minimized.
In Which Situations Is Tracheal Stent Used?
Stent usage areas are grouped under two main headings according to whether the disease is benign or malignant.
Airway Obstructions Due to Malignant Tumors
Lung cancer, esophageal cancer, or thyroid cancers can directly attack the trachea or block the airway by pressing externally.
In such oncological cases, the stent opens the blockage created by the tumor, allowing the patient to become stable enough to receive radiotherapy or chemotherapy.
Stent application in palliative care helps the patient to breathe comfortably and maintain their quality of life even in the last stages.
Benign Strictures and Tracheomalacia (Tracheal Softening)
Patients who are intubated for a long time in intensive care (put to sleep with a tube in the trachea) may develop “post-intubation stenosis” due to the pressure created by the tube.
Tracheomalacia, on the other hand, is a condition in which the tracheal cartilages soften and stick together with each inhalation.
In such cases, a stent is preferred as a permanent or temporary solution in patients where surgical repair is risky.
What are the Types of Tracheal Stents?
The material of the stent to be used should be carefully selected by the specialist physician according to the patient’s diagnosis and life expectancy.
Silicone Stents (Dumont Stent) and Their Advantages
Silicone stents are devices made of biocompatible medical silicone and are generally preferred in benign stenosis.
- Texture Harmony: It has a low risk of reacting with surrounding tissues and has little tendency to form granulation (excessive flesh growth) tissue.
- Removability: They can be easily removed with rigid bronchoscopy when they are no longer needed or need cleaning.
- Cost: They are more economical than metallic stents, but rigid bronchoscopy and general anesthesia are absolutely required for their placement.
Self-Expanding Metallic Stents (Nitinol Stent)
Made of nitinol (nickel-titanium mixture) material, these stents have a memory structure and open spontaneously where they are placed.
They are often used to accommodate the pressure of malignant tumors because they have much thinner walls and provide a larger inner diameter than silicone stents.
Covered metallic stents are covered with a special polymer layer that prevents the tumor from growing through the pores of the stent.
Hybrid Stent Designs
Hybrid stents are modern designs that combine both the tissue-friendly properties of silicone and the flexibility of metal.
These models, which adapt to the shape of the trachea (such as the Y stent), are especially preferred in stenosis (carina) at the separation point of the main bronchi.
How is a Tracheal Stent Inserted? Application Process
Stent placement is an advanced interventional bronchoscopy procedure that requires high experience and specialized equipment.
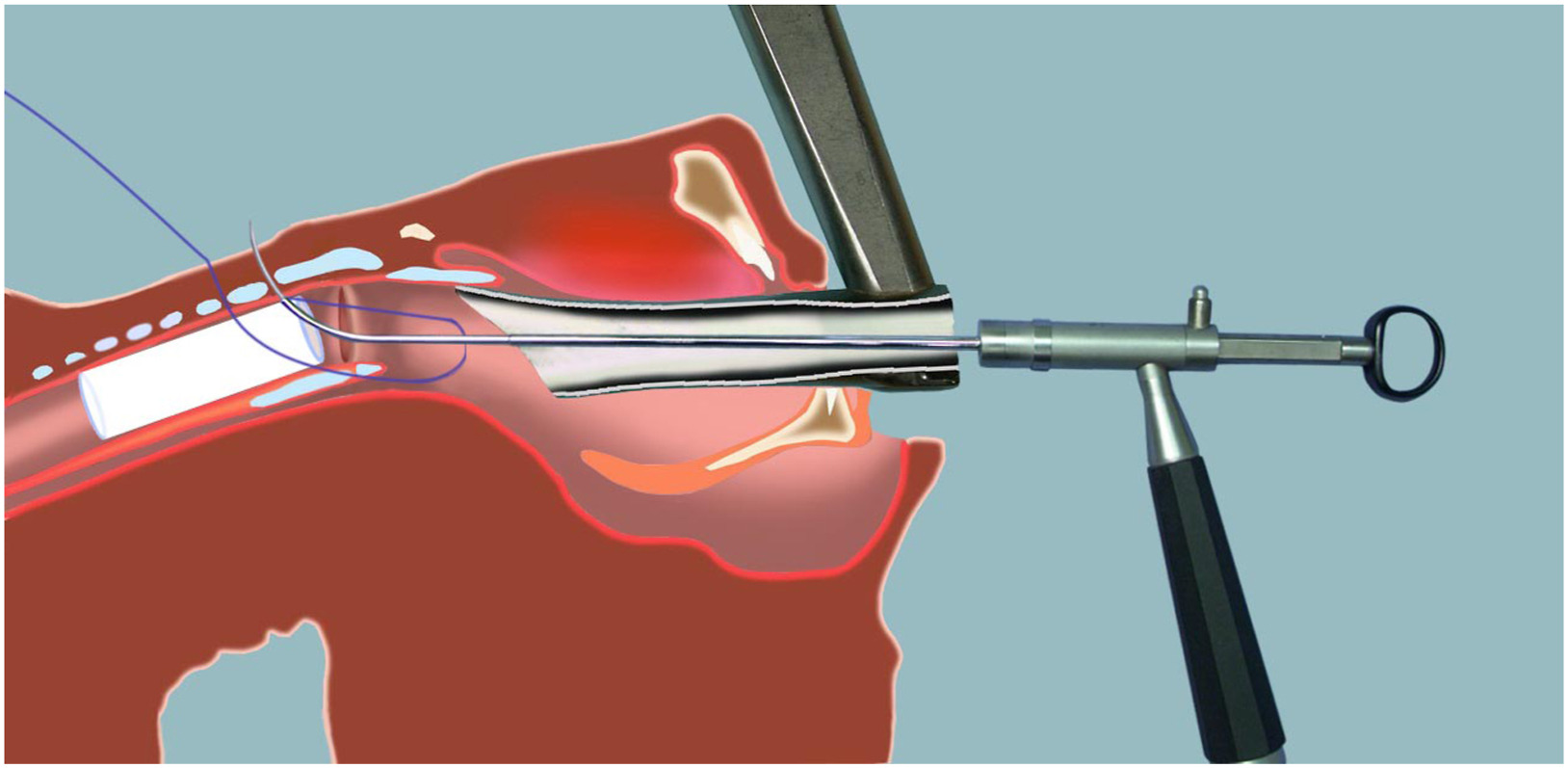
Stent Placement Under Rigid Bronchoscopy
Rigid bronchoscopy is a metal, tubular device that is inserted through the patient’s mouth and into the windpipe.
This method offers the surgeon a wide working area and allows silicone stents to be folded and placed in the stenosis area.
After the stent is placed, the position of the stent is checked millimetrically through the bronchoscope to ensure full patency.
Preparation and Anesthesia Before Stent Application
Before the procedure, the patient’s tomography and bronchoscopic images are examined and the length and diameter of the stricture are measured.
The operation is performed under general anesthesia and in a fully equipped operating room.
The patient does not feel any pain or shortness of breath because he is completely asleep during the procedure; The operation time is usually between 30-60 minutes.
Advantages of Tracheal Stent Application and Expected Results
A stent placed at the right time and with the right technique can change the patient’s clinical picture in minutes.
Immediate relief from shortness of breath
As soon as the stent is placed and the bronchoscope is removed, the patient can take a deep breath as soon as he wakes up, as the area of stenosis is completely opened.
This rapid recovery allows the patient to leave the intensive care unit or be weaned off the ventilator (weaning).
Increased Quality of Life and Effort Capacity
Patients who become bedridden because they cannot breathe can take short-distance walks after the stent and do their daily work on their own.
Especially in cancer patients, stents also provide psychological relief by eliminating the panic caused by shortness of breath and the fear of dying.
Comparison Table of Stent Types
| Feature | Silicone Stent | Metallic (Nitinol) Stent |
| Placement Method | Rigid Bronchoscopy (Operating Room) | Flexible Bronchoscopy (Clinical) |
| Tissue Reaction | Very Low | Higher |
| Removable | It’s easy | Hard (Gets harder as time goes on) |
| Main Usage Area | Benign Strictures / Before Surgery | Malignant Tumors (Palliative) |
| Risk of Granulation | Low | Medium-High |
Prof. Dr. Levent Alpay: Tracheal stent application is one of the most critical interventions in thoracic surgery. The important thing here is not only to insert the stent, but also to choose the type of stent that best suits the patient’s anatomy and the course of the disease. We blend the advantage of silicone stents being removable with the expansion power of metallic stents with the right case selection. It should not be forgotten that; The stent is not a goal, but a tool that allows the patient to breathe comfortably and continue their original treatment.
Case Experience (Anonymous):
Our 65-year-old patient, whose main trachea narrowed by 80% due to advanced lung cancer, was admitted to our emergency department with severe respiratory failure. In the emergency intervention performed with rigid bronchoscopy, a 14 mm diameter coated metallic stent was placed in the area under tumor pressure. The patient, whose bruising recovered after the procedure and his breathing returned to normal, recovered enough to start radiotherapy treatment a day later.
If you complain of shortness of breath due to tracheal stenosis, you can make an appointment with our clinic for stent application and personalized treatment planning and seek expert opinion.
Post-Stent Care and Follow-up Process
Regular monitoring of the patient after stent placement is vital to ensure that the stent does not become blocked or displaced.
Stent Cleaning and Moisturizing Recommendations
A stent is a foreign substance to the body and can cause phlegm (mucus) accumulation on it.
Patients are advised to perform regular saline inhalation (steam therapy) and drink plenty of fluids; In this way, the sputum remains soft and easily expelled from the stent.
Possible Complications: Displacement and Mucus Obstruction
- Migration: The stent can sometimes be replaced by a severe cough; In this case, it must be corrected by bronchoscopy again.
- Mucus Plug: Thick sputum can block the inside of the stent; If this leads to immediate shortness of breath, bronchoscopic cleaning is essential.
- Meat Growth: Flesh growths may occur at the ends of the stent with the body’s reaction; These tissues are cleaned by laser or freezing (cryo) method.
Frequently Asked Questions
How Long Can a Tracheal Stent Stay in the Body?
Silicone stents can remain in the body for years, but it is recommended to check them every 6-12 months or replace them if necessary. Metallic stents are generally designed to remain in malignant diseases for life.
Is Speech or Swallowing Affected After Stent Placement?
Since the stent is placed under the vocal cords, it does not affect speech; However, a short-term hoarseness is normal immediately after the procedure. Stents large enough to compress the esophagus can rarely cause swallowing difficulties.
Can the Inserted Stent Be Removed Later?
Silicone stents are always removable. While coated metallic stents can be easily removed within the first few months, open metallic stents are much more difficult to remove due to their fusion into tissue.
Scientific Bibliography
- Journal of Thoracic Disease: Evolution of Tracheal Stents and Current Trends
- PubMed (NCBI): Complications of Tracheal Stenting in Benign and Malignant Diseases
- Chest (Official Journal of the American College of Chest Physicians): Guidelines for Interventional Pulmonology
- Turkish Thoracic Society: A Guide to Interventional Bronchoscopy and Stent Applications
